The debate over fluoride in America’s drinking water has moved from fringe concern to mainstream policy battle, and the consequences for children’s teeth are now quantified.
Researchers at Harvard School of Dental Medicine and Brigham and Women’s Hospital published a modeling study in JAMA Health Forum projecting that eliminating fluoride from public water systems nationwide would produce more than 25 million additional decayed teeth in children within five years, at an added cost of $9.8 billion in dental treatment.
As of early 2026, more than 15 states have introduced legislation to restrict or ban water fluoridation, following Florida and Utah’s enactment of statewide bans in 2025.
For Queens families, whose tap water is still fluoridated at the recommended 0.7 mg/L, this national battle has direct implications for what protective steps you take and what happens if the policy landscape shifts.
WHAT YOU NEED TO KNOW
- Where things stand: Florida and Utah enacted statewide fluoride bans in 2025. More than 15 other states introduced ban legislation in 2026. New Jersey is advancing protections for fluoridation.
- The cost of removing fluoride: A Harvard/JAMA study projects 25.4 million additional decayed teeth in children over five years if fluoride is removed nationally, costing $9.8 billion. Low-income Medicaid-enrolled children bear the greatest impact.
- EPA action: The EPA launched an accelerated review of fluoride in drinking water on February 6, 2026, following a 2024 federal court ruling.
- FDA action: The FDA limited ingestible fluoride supplement prescriptions for children age 3 and younger in October 2025.
- Queens/NYC status: New York City continues to fluoridate its water at the recommended 0.7 mg/L. No ban legislation has advanced in New York State.
What Is Happening With Fluoride Policy Right Now
Community water fluoridation has been a standard US public health practice since 1945 and currently reaches approximately 70% of the US population.
It has been endorsed by the American Dental Association, the American Academy of Pediatrics, the CDC, the World Health Organization, and the American Medical Association.
The CDC has called it one of the ten great public health achievements of the 20th century.
According to the ADA, fluoridated water at the optimal level of 0.7 mg/L reduces tooth decay by 25% in both children and adults.
That consensus is now under direct political pressure.
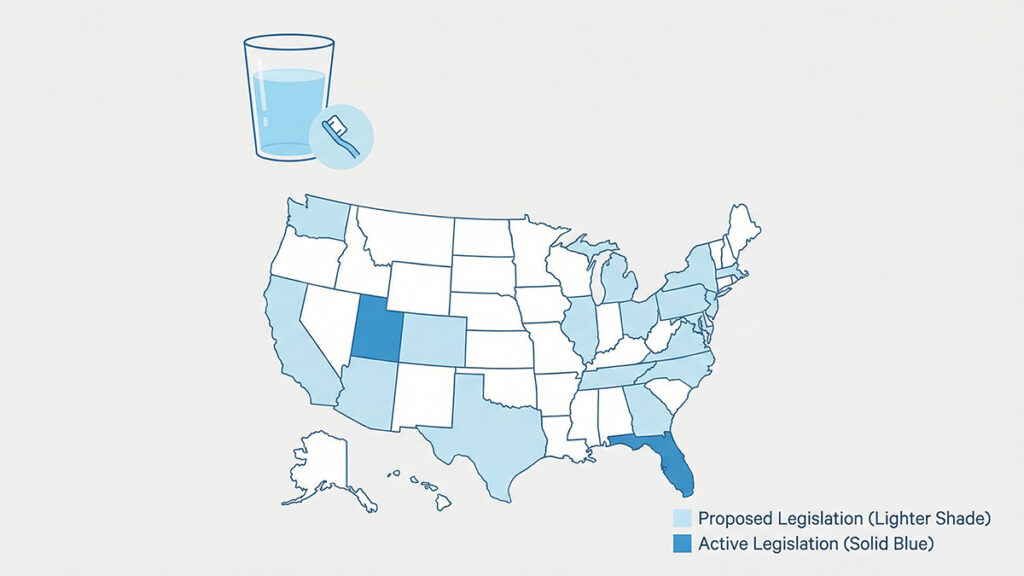
In 2025, Florida and Utah became the first states to enact statewide bans on community water fluoridation.
In 2026, the movement accelerated rapidly.
According to CareQuest Institute for Oral Health, which tracks fluoridation legislation in real time, more than 15 states introduced bills in early 2026 to restrict or ban fluoridated water, described by CareQuest’s senior public policy director Melissa Burroughs as “a much heavier load in terms of these statewide actions on fluoride compared to last year.”
At the federal level, the EPA announced on February 6, 2026, that it will initiate an accelerated review of fluoride in drinking water under the Safe Drinking Water Act.
This review follows a 2024 federal court ruling that directed the EPA to strengthen its assessment of potential fluoride risks.
EPA Administrator Lee Zeldin stated he is “working in lockstep” with HHS Secretary Robert F. Kennedy Jr., who has said that “a growing body of evidence indicates that ingesting fluoride can cause neurological harm.”
ADA President Richard Rosato responded that the ADA is “hopeful that the EPA will use peer-reviewed, scientifically tested evidence rather than biased, mischaracterized studies.”
To understand what fluoride actually does for your child’s teeth and how it works, our complete guide to fluoride in children’s dental health explains the science in plain language.
What the Harvard/JAMA Study Actually Projects
The most significant new data point in this debate comes from a modeling study published in JAMA Health Forum by researchers Sung Eun Choi, PhD, of Harvard School of Dental Medicine, and Lisa Simon, MD, DMD, of Brigham and Women’s Hospital.
The study modeled the projected impact of removing fluoride from public water systems across the United States.
The findings are stark. Eliminating community water fluoridation (CWF) nationally would:
- Increase tooth decay in children by 7.5 percentage points over five years
- Produce an estimated 25.4 million additional decayed teeth in children within five years
- Generate $9.8 billion in additional dental treatment costs over five years
- Place the greatest financial burden on low-income and uninsured families, the populations least able to afford alternative preventive care
CareQuest Institute published a complementary analysis focused on the state level, finding that eliminating CWF in just five states would result in 132,000 additional children developing cavities and nearly $40 million in added Medicaid costs within three years.
The state-level analysis is critical context: even partial implementation of fluoride bans creates measurable harm concentrated in Medicaid-enrolled children, the same children who already face the greatest barriers to dental access, as documented in the recent surge in kids’ ER visits for preventable tooth pain.
The ADA has noted the JAMA study “should be considered exploratory” while reaffirming its support for community water fluoridation.
To date, the ADA states it has seen “no peer-reviewed research that would change its long-standing recommendation to the public to brush twice a day with fluoride toothpaste and drink optimally fluoridated water.”
Our complete guide to cavities in children covers all the cavity prevention tools available, including alternatives to water fluoridation for families in non-fluoridated areas.
The FDA Fluoride Supplement Restriction: What Parents Need to Know
Separate from the water fluoridation debate, the FDA took action in October 2025 to limit ingestible fluoride prescription drug products for children age 3 and younger.
For children at high caries risk who are older than 3, the FDA continues to advise fluoride supplements with physician oversight.
This is significant because fluoride supplements are the primary alternative for children in non-fluoridated areas, precisely the children who most need supplemental fluoride protection if water fluoridation is removed.
The ADA's response was pointed: "If prescription and over-the-counter fluoride supplements are also banned, then there are fewer prevention methods of tooth decay available."
In states like Utah and Florida, where water fluoridation has already been banned, families now face a narrowed toolkit; water fluoridation is gone, and ingestible supplements are restricted for toddlers.
The remaining options for children in non-fluoridated areas include fluoride toothpaste (recommended for all children from the first tooth), professional fluoride varnish applications at dental visits, fluoride in dentist-prescribed rinses for older children, and silver diamine fluoride, a topical treatment that both arrests existing cavities and prevents new ones, now gaining wider adoption precisely because of the fluoride policy uncertainty.
Queens and New York City: What Is the Current Status?
Queen’s parents can take some reassurance from the current local picture.
New York City continues to fluoridate its drinking water at 0.7 mg/L, the level recommended by the US Department of Health and Human Services.
No ban legislation has advanced in New York State.
In fact, neighboring New Jersey has moved in the opposite direction, advancing legislative protections for community water fluoridation as other states debate bans.
However, the federal EPA review now underway could ultimately result in new national regulations that affect New York regardless of state-level decisions.
If the EPA were to set a maximum contaminant level for fluoride that is incompatible with current community fluoridation standards, municipalities, including New York City, could be required to reduce or eliminate fluoride in their water systems not by state choice, but by federal regulatory mandate.
This is not a certain outcome.
The EPA review process typically takes years, and the ADA, AAPD, and more than 140 health and dental organizations have submitted formal comments challenging the scientific rigor of the EPA’s planned assessment methodology.
But Queens’ parents should understand that the current fluoride policy landscape is the most contested it has been in decades.
The practical implication is simple: don’t rely on any single fluoride source.
Fluoride toothpaste, twice daily, with fluoride varnish at every dental visit, provides meaningful protection regardless of what happens to water fluoridation policy.
To find a Queens pediatric dentist who applies fluoride varnish at checkups, browse our Queens pediatric dentist directory.
What This Means for Your Child By Age
Infants and toddlers (under age 3): The FDA’s October 2025 action limits ingestible fluoride supplement prescriptions for children in this age group. For families in fluoridated areas like Queens, this change is largely academic; your child is already receiving fluoride through tap water and, once teeth erupt, through fluoride toothpaste. The AAPD recommends a rice-grain-sized amount of fluoride toothpaste from the first tooth and a pea-sized amount from age 3. Use fluoridated tap water for mixing formula and drinking rather than filtered water that may have fluoride removed.
Ages 3–6: This is the highest-risk window for early childhood caries. Children in this age group benefit most from community water fluoridation because they consume large amounts of water relative to body weight and are in the cavity-prone baby teeth years. If you live in a fluoridated area, using tap water for drinking and cooking provides passive, consistent fluoride exposure that protects teeth throughout the day at zero cost and zero effort.
Ages 6–12: Permanent teeth are erupting. Fluoride’s protective role shifts from preventing early childhood caries to mineralizing and hardening newly erupted enamel, making permanent teeth more resistant to decay for life. Children who consume optimally fluoridated water during the years when permanent teeth are forming benefit from a structural advantage in their enamel that persists into adulthood. This is also the window when dental sealants on first permanent molars add a second layer of mechanical protection on top of fluoride’s chemical protection.
All ages: The single most reliable fluoride source in any policy environment is fluoride toothpaste, used twice daily. Unlike water fluoridation, which can be changed by legislative or regulatory action, fluoride toothpaste remains widely available, inexpensive, and effective. The CDC and ADA both endorse its use from the first tooth. Whatever happens to water policy, this habit remains constant.
Frequently Asked Questions About Fluoride Bans and Children’s Teeth
Does New York City’s water have fluoride in it?
Yes. New York City fluoridates its public water supply at 0.7 mg/L, the level recommended by the US Department of Health and Human Services.
This is true as of March 2026. No ban legislation has advanced in New York State.
Parents can verify current NYC water fluoride levels at the NYC Department of Environmental Protection website.
Should I give my child fluoride supplements if they mostly drink bottled water?
Possibly, but this requires a conversation with your child’s pediatric dentist. Most bottled water does not contain fluoride.
If your child drinks primarily bottled water and is at elevated cavity risk, your pediatric dentist may recommend fluoride supplements for children over age 3 or topical fluoride varnish at dental visits to compensate.
For children under 3, the FDA’s 2025 action limits ingestible fluoride supplements.
Ask your pediatric dentist for guidance specific to your child’s age and cavity risk.
Is fluoride in water really safe for children?
At the level used for community water fluoridation (0.7 mg/L), the overwhelming consensus of US and international health organizations, including the CDC, WHO, ADA, AAP, and American Medical Association, is that fluoridated water is safe and effective for children.
Concerns about neurological effects, cited by RFK Jr. and others, are primarily based on studies of populations with exposure to fluoride at levels far higher than those used in US water systems (some studies involved populations exposed to naturally occurring fluoride at 2–10+ mg/L).
The scientific debate is about whether current review processes are using the best available research, not about whether there is established harm at US fluoridation levels.
The ADA continues to recommend fluoridated water for children and adults.
What should I do if my state bans fluoride in water?
Queens and New York City parents are not currently affected by any state-level fluoride ban.
If you live in a state that has enacted a ban, or if policy changes in the future: maintain twice-daily brushing with fluoride toothpaste; ask your pediatric dentist about professional fluoride varnish at every 6-month visit; consider whether your child qualifies for fluoride supplements (for children over age 3); ensure your child’s molars receive dental sealants; and limit added sugar consumption to reduce cavity-causing bacterial activity.
Medical disclaimer: This article is for informational purposes only and does not constitute medical or dental advice. Fluoride recommendations may evolve as research and policy develop. Always consult a licensed pediatric dentist for guidance specific to your child's age, cavity risk, and local water fluoridation status.
Reviewed by the Pediatric Dentist in Queens Editorial Team. Last Updated: March 17, 2026.
9. SOURCE LIST
1. JAMA Health Forum “Projected Impact of Removing Fluoride from Public Water Systems in the United States.” Sung Eun Choi, PhD; Lisa Simon, MD, DMD. Published May 30, 2025. https://jamanetwork.com/journals/jama-health-forum/fullarticle/2834515
2. CareQuest Institute “New Study Shows Costly Consequences for States Banning Fluoride.” December 2025. https://carequest.org/new-study-shows-costly-consequences-for-states-banning-fluoride/
3. CareQuest Institute “Fluoride at a Crossroads: What the EPA’s New Review Means.” February 5, 2026. https://carequest.org/fluoride-at-a-crossroads-what-the-epas-new-review-means-and-why-it-matters/
4. CareQuest Institute “The New Fault Lines on Fluoride in Four States.” February 2026. https://www.carequest.org/about/blog-post/new-fault-lines-fluoride-four-states-and-what-they-mean-medicaid
5. Axios “Fluoride ban efforts show RFK Jr.’s reach.” February 2, 2026. https://www.axios.com/2026/02/02/fluoride-ban-water-kennedy-rfk-epa
6. ADA “EPA initiates accelerated review of fluoride in drinking water.” February 6, 2026. https://adanews.ada.org/ada-news/2026/february/epa-initiates-accelerated-review-of-fluoride-in-drinking-water/
7. ADA “ADA urges EPA to strengthen scientific rigor in fluoride health assessment.” February 25, 2026. https://adanews.ada.org/ada-news/2026/february/ada-urges-epa-to-strengthen-scientific-rigor-in-fluoride-health-assessment/
8. ADA “Statement on FDA Action to Remove Ingestible Fluoride Prescription Drug Products.” October 31, 2025. https://www.ada.org/about/press-releases/statement-from-the-ada-on-fda-action-to-remove-ingestible-fluoride-prescription-drug-products
NOTE: The JAMA Health Forum study was published May 30, 2025, but received major media coverage and became the central data point in the 2026 state fluoride ban debate. It is cited in the article with its original publication date and framed as the key evidentiary backdrop to the current policy debateThe debate over fluoride in America’s drinking water has moved from fringe concern to mainstream policy battle, and the consequences for children’s teeth are now quantified.

Mary – Queens Pediatric Dental Resource Manager. I’m a dental health researcher and parent advocate based in Queens, NY. After struggling to find reliable pediatric dental information during my own child’s dental emergency, I created this resource to help other Queens families navigate their children’s oral health needs.
I curate evidence-based information from leading pediatric dental organizations, peer-reviewed research, and trusted dental health experts. While I’m not a dentist, I’m committed to providing accurate, practical guidance that helps parents make informed decisions.
All content is thoroughly researched and includes proper medical disclaimers directing families to consult qualified pediatric dentists for their children’s specific needs.