Reviewed by our dental health editorial team. Last Updated: March 2026.
Quick Answer: A March 2026 study from the University of Copenhagen analyzed health records from 568,000 children and found that kids with multiple cavities had up to 45% higher incidence of cardiovascular disease as adults. Kids with severe gingivitis had up to 41% higher incidence. The study does not prove cavities cause heart disease, but it identifies a meaningful statistical link that gives parents one more important reason to stay on top of their child’s dental care. Prevention brushing, fluoride, and regular dental visits remain the clearest action step.
You already know cavities hurt.
They cause toothaches, require fillings, and can affect how your child eats, sleeps, and focuses in school.
Now, a major new study suggests the consequences of childhood tooth decay may extend far beyond the dentist’s office, all the way to your child’s heart health decades from now.
On March 2, 2026, researchers at the University of Copenhagen published findings from one of the largest studies ever conducted on childhood oral health and long-term disease outcomes.
By tracking the dental records and adult health outcomes of more than half a million Danish children, they found a striking statistical association between childhood cavities and gum disease and the later development of heart attacks, strokes, and type 2 diabetes.
This is genuinely important research.
It is also research that requires careful interpretation because correlation is not causation, and the headline numbers need context to be useful for parents.
This article explains exactly what the researchers found, what it does and does not mean, and what parents in Queens and across the country can do about it today.
For background on why cavities form in the first place, our complete guide to cavities in children covers risk factors, prevention, and treatment options at every age.
Key Takeaways
- 568,000 children studied: The University of Copenhagen analyzed dental records from 568,778 Danish children born between 1963 and 1972, tracking their health outcomes through 2018 when they were 30 to 56 years old.
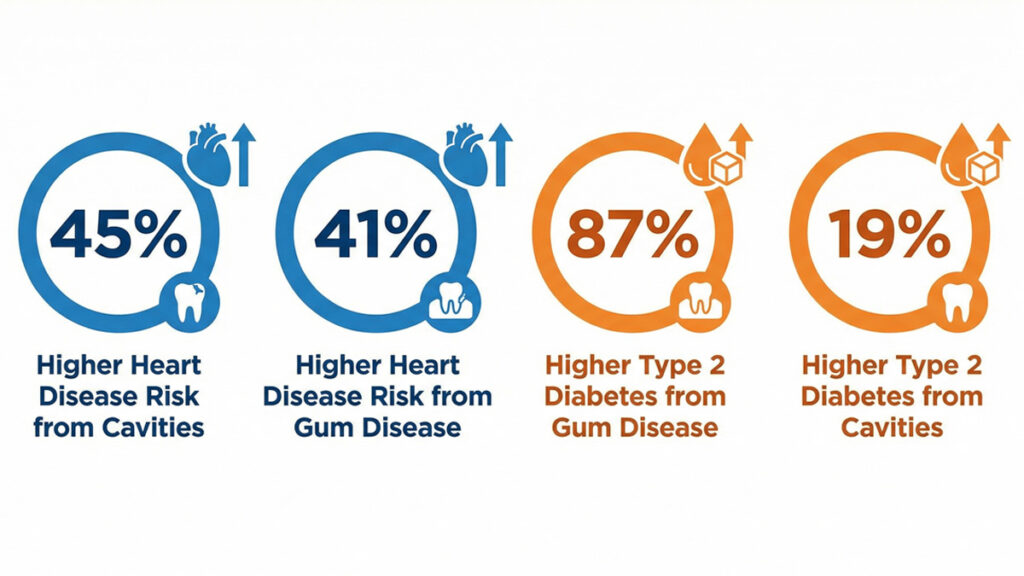
- Cavities linked to 45% higher heart disease incidence: Children with numerous tooth cavities had up to 45% higher incidence of cardiovascular disease, including heart attack, stroke, and coronary artery disease, compared to children with few cavities.
- Gum disease carries similar risk: Children with severe gingivitis showed up to 41% higher incidence of cardiovascular disease. Risk increased as the severity of dental problems worsened.
- Diabetes connection is striking: A companion study by the same researchers found children with severe gum disease had up to 87% higher incidence of type 2 diabetes in adulthood. Multiple cavities were associated with 19% higher incidence.
- Association, not proof of cause: The study identifies a statistical correlation. Researchers explicitly state they did not investigate causes; they cannot say cavities cause heart disease. But the pattern held even after adjusting for socioeconomic factors.
- What this means for parents: Preventing cavities and gum disease in childhood is even more important than previously understood. Regular dental visits, fluoride toothpaste, and good brushing habits are the clearest preventive steps available today.
Why Is This Study Getting So Much Attention?
Published on March 2, 2026, in the International Journal of Cardiology, the University of Copenhagen study is generating significant coverage because of its extraordinary scale and its long follow-up period.
Most studies linking oral health to systemic disease are conducted in adults.
This one started with children tracking their dental health from routine childhood dental visits, then following them into middle age to see what diseases they developed.
The research was covered by EurekAlert, Medical Xpress, News-Medical, and science outlets worldwide within days of publication.
Parents in Reddit communities, including r/Mommit, r/beyondthebump, and r/Parenting, began sharing headlines with understandably alarmed reactions: “Does this mean my kid’s cavities will give them a heart attack?”
The short answer is no, the research does not say that, and we will explain why.
But the longer answer is that this study adds meaningful weight to something dental researchers have suspected for years: oral health and systemic health are more connected than most people realize.
What Did the University of Copenhagen Study Actually Find?
The study, led by Nikoline Nygaard, a postdoctoral researcher at the University of Copenhagen’s Department of Odontology, and co-authored by Associate Professor Merete Markvart, is a nationwide cohort study, one of the most methodologically rigorous designs in epidemiological research.
Here is how it worked: the researchers pulled dental health data from Denmark’s National Child Odontology Registry for all children born between 1963 and 1972 who had at least two recorded dental visits, totaling 568,778 individuals.
They then cross-referenced those dental records with cardiovascular and other disease diagnoses from Denmark’s National Patient Register covering 1995 through 2018.
By that point, the participants were between 30 and 56 years old.
The findings, as reported on the University of Copenhagen’s official news site, showed clear patterns:
- Children with numerous tooth cavities had up to 45% higher incidence of cardiovascular disease, including heart attack, stroke, and coronary artery disease, compared to children with few cavities
- Children with severe gingivitis showed up to 41% higher incidence of cardiovascular disease
- Risk appeared to increase as the severity of dental problems during childhood worsened
- The pattern held for both boys and girls, though the exact figures varied by sex
- Results were adjusted for educational level, a standard proxy for socioeconomic status, and lifestyle factors such as diet, exercise, and healthcare access, and the association remained strong even after that adjustment
A companion study by the same research team looked at type 2 diabetes and found an even more pronounced pattern: children with severe gum disease had up to 87% higher incidence of type 2 diabetes in adulthood, while those with multiple cavities had 19% higher incidence.
“We suspect that exposure to high levels of inflammation in the form of gum disease and dental caries already in childhood may influence how the body later responds to inflammation.” Nikoline Nygaard, Postdoctoral Researcher, University of Copenhagen Department of Odontology
Why Might Cavities and Gum Disease Be Connected to Heart Health?
The researchers are careful to note that this study identified correlations and statistical associations, but did not investigate the underlying biological causes.
They cannot say based on this study alone that cavities cause heart disease.
That distinction matters enormously, and it is one that many news headlines have blurred.
That said, the researchers and the broader scientific community have a leading theory: chronic inflammation.
The inflammation pathway works like this: cavities and gum disease are both driven by bacterial infection.
When bacteria colonize the gums and dental tissue, the immune system responds with inflammation.
In children with persistent, untreated dental disease, that inflammatory response becomes chronic and widespread, affecting not just the mouth but potentially the entire body’s immune and vascular systems.
Over years and decades, chronic systemic inflammation is one of the primary mechanisms behind atherosclerosis, the hardening and narrowing of arteries that leads to heart attack and stroke.
Researchers hypothesize that early and prolonged exposure to inflammation from dental disease may alter how the body responds to inflammatory signals throughout life.
This theory has broader scientific support.
The World Heart Federation has published a consensus report stating that strong evidence exists that periodontitis, advanced gum disease in adults, increases the risk of cardiovascular disease.
Research suggests that bacteria from infected gums can enter the bloodstream directly and trigger inflammatory responses elsewhere in the body, accelerating atherosclerotic disease.
The Copenhagen study extends this concern earlier in life to childhood dental health.
“It’s not that you can solve cardiovascular disease by treating children’s teeth. But if we target our efforts towards specific groups, you can nudge many people in the right direction simply by improving their oral health.” Merete Markvart, Associate Professor, University of Copenhagen Department of Odontology
It is also important to acknowledge that shared risk factors likely play a role.
Children who grow up in households with limited healthcare access, high-sugar diets, and lower socioeconomic resources tend to have both more dental disease and more cardiovascular risk factors as adults.
The Copenhagen researchers adjusted for educational level, and the association persisted, suggesting oral health contributes independently, but they acknowledge that lifestyle cannot be fully ruled out as a contributing factor.
What Does This Mean for Children in the US?
Denmark has a nationally integrated public dental care system for children, meaning the data captured routine dental visits for essentially all children born in those birth years.
The US context is different.
Access to pediatric dental care is significantly more uneven, with lower-income children, Medicaid-enrolled children, and children in underserved communities facing far greater barriers to routine dental care.
Tooth decay is already the most common chronic disease of childhood in the United States.
According to the CDC, more than half of children ages 6 to 8 have had a cavity in a primary tooth, and nearly 60% of adolescents ages 12 to 19 have had a cavity in a permanent tooth.
If the Copenhagen findings translate to US populations, and researchers believe they likely do, the long-term public health implications are substantial.
In communities like Queens, New York, where pediatric dental access varies significantly by neighborhood and insurance status, this research reinforces the urgency of early and consistent preventive dental care.
The populations with the highest cavity burden in childhood are the same populations already at elevated cardiovascular risk in adulthood.
That overlap is not coincidental.
Our guide to your child’s first dental visit covers when to start dental care and what to expect, because for many families, the first visit is the hardest step.
Does My Child’s Past Cavity History Mean They Are at Risk?
This is the question most parents will immediately ask, and it deserves a careful, honest answer.
This study looked at population-level patterns across hundreds of thousands of children over decades.
It cannot tell you what will happen to your specific child.
A single cavity at age 7 does not predict a heart attack at age 47.
The study examined children with numerous cavities and severe gingivitis patterns of persistent, significant dental disease, not isolated incidents of tooth decay that were promptly treated.
Importantly, the research tracked children through 2018 using health data from the 1960s and 1970s, a period when childhood dental care and treatment options were considerably less advanced than they are today.
Children who had untreated dental disease for years would have had far greater chronic bacterial load and inflammation than children who receive modern preventive care, including fluoride varnish, dental sealants, and early intervention.
What this research does mean is that consistently poor oral health over childhood, the pattern of recurring, untreated, or inadequately managed dental disease is associated with measurably worse long-term outcomes.
That is a reason to take your child’s dental health seriously starting now, not a reason to panic about what has already happened.
If your child has had cavities, the most productive response is to work with your pediatric dentist to address them promptly and establish strong prevention habits going forward.
For children with early decay, our guide to silver diamine fluoride explains a non-drilling treatment option that stops cavity progression and is increasingly used in pediatric dental offices.
What Expert Organizations Say About the Oral-Systemic Connection
The Copenhagen study is groundbreaking in its scale and its childhood focus, but it builds on a body of research that professional health organizations have been monitoring for years.
The American Academy of Pediatric Dentistry has long recognized the oral-systemic connection in its clinical guidelines, emphasizing that the mouth is not separate from the rest of the body and that chronic oral infections in children can have systemic consequences.
The AAPD’s preventive dentistry guidelines, including twice-daily brushing with fluoride toothpaste, twice-yearly fluoride varnish applications, and dental sealants for high-risk children, are designed precisely to eliminate the chronic bacterial burden that the Copenhagen researchers identified as the likely mechanism behind the long-term risk.
The American Heart Association has published research connecting adult periodontal disease to cardiovascular risk.
This new study from Copenhagen extends that concern to childhood oral health and does so with a dataset large enough to command serious attention from both the dental and medical communities.
Understanding the full picture of why fluoride and preventive dental care matter for children is even more compelling in light of this research.
What Should Parents Do Right Now?
Start preventive care as early as possible
The AAPD recommends a child’s first dental visit by age 1 or within six months of the first tooth appearing.
Early visits establish a dental home, identify early decay, and give your dentist the opportunity to apply protective fluoride varnish before problems develop.
Brush twice daily with fluoride toothpaste every day, not most days
The Copenhagen study identified persistent dental disease as a risk factor.
Consistent daily brushing with the right amount of fluoride toothpaste for your child’s age is the single most effective thing you can do.
Our kids oral hygiene guide covers the age-by-age routine in full.
Do not ignore gingivitis
One of the most important findings in the Copenhagen research was that swollen, bleeding gums due to gingivitis carried cardiovascular risk comparable to cavities.
Professor Markvart specifically called for more research attention to gingivitis, noting that it is significantly under-recognized in children.
If your child’s gums bleed when they brush, that is not normal.
It is a sign of gum inflammation that needs to be addressed at a dental visit.
Ask about dental sealants for back teeth
Dental sealants are a thin protective coating applied to the biting surfaces of back molars, the teeth most vulnerable to decay.
The CDC reports that sealants prevent approximately 80% of cavities in back teeth for the first two years and nearly 50% for up to four years.
For children at elevated cavity risk, sealants are one of the highest-impact preventive interventions available.
Keep the six-month dental schedule
Early detection and treatment of cavities and gum disease means less chronic bacterial exposure over childhood, and based on what this study found, that matters far beyond your child’s smile.
The Bottom Line on Childhood Cavities and Heart Disease
The University of Copenhagen’s March 2026 study of 568,000 children is the largest of its kind and adds significant weight to the growing understanding that childhood oral health shapes long-term systemic health.
Children with numerous cavities or severe gingivitis showed up to 45% higher incidence of cardiovascular disease and up to 87% higher incidence of type 2 diabetes as adults, even after adjusting for socioeconomic factors.
The study does not prove cavities cause heart attacks, but the association is real, large in scale, and consistent with what researchers already understand about chronic inflammation and cardiovascular risk.
The actionable message for parents is not an alarm; it is an urgency about prevention.
Brushing twice daily with fluoride toothpaste, attending dental visits every six months, treating decay promptly, and taking bleeding gums seriously are all within reach for most families.
These steps protect your child’s teeth today.
If this research holds up in future studies, they may also be protecting your child’s heart for decades to come.
This article provides general information about the relationship between childhood oral health and systemic disease risk. It does not replace professional dental or medical advice. Always consult your child’s pediatric dentist or physician before making health decisions.
Frequently Asked Questions About Childhood Cavities and Heart Disease Risk
Does this study prove that cavities cause heart disease?
No. The University of Copenhagen study is a cohort study that identified statistical associations, not causal relationships.
The researchers explicitly state they did not investigate biological causes, only patterns in population data.
The findings show a significant correlation that is consistent with existing inflammation-based theories, but correlation alone does not establish cause and effect.
Further research is needed to determine whether and how childhood oral health directly influences long-term cardiovascular outcomes.
My child has had a few cavities. Should I be worried about their heart health?
No cause for panic.
The study focused on children with numerous cavities and severe gingivitis over childhood patterns of persistent, significant dental disease.
A single cavity or two that were promptly treated is a very different situation from the chronic, widespread dental disease that showed the strongest associations in the data.
The right response is to ensure cavities are treated promptly and to build strong prevention habits going forward.
Why was the diabetes risk even higher than the heart disease risk?
In the companion study, children with severe gum disease showed up to 87% higher incidence of type 2 diabetes, a larger statistical association than the cardiovascular finding.
Researchers believe this may reflect the overlap between chronic inflammation, insulin resistance, and metabolic disease.
Periodontal bacteria and inflammatory markers associated with gum disease are also implicated in disrupting glucose metabolism.
This is an active area of research in both adult and pediatric populations.
Do children in the US have worse cavity rates than in Denmark?
Yes, in many populations.
The US has significant disparities in pediatric dental access based on income, insurance status, and geography.
According to the CDC, more than half of children ages 6 to 8 have already had a cavity.
In Denmark, a nationally integrated public dental system provides universal access to childhood dental care, meaning this study’s findings likely underrepresent what might be found in high-risk US populations with less consistent dental care access.
What is gingivitis in children, and how do I know if my child has it?
Gingivitis is inflammation of the gums caused by bacterial plaque buildup at the gum line.
In children, signs include gums that appear red or swollen rather than pink and firm, and gums that bleed during brushing or flossing.
Many parents assume bleeding gums during brushing is normal it is not.
Healthy gums should not bleed with regular, gentle brushing. If your child’s gums bleed consistently, bring it up at the next dental visit.
How do dental sealants help reduce cavity risk?
Dental sealants are thin protective coatings applied by a dentist to the biting surfaces of back molars, where deep grooves trap food and bacteria that brushing cannot always reach.
The CDC reports sealants prevent approximately 80% of cavities in back teeth for the first two years after application.
Children ages 6 to 14, when the first and second permanent molars come in, benefit most from sealants. Ask your pediatric dentist whether your child is a candidate.

Mary – Queens Pediatric Dental Resource Manager. I’m a dental health researcher and parent advocate based in Queens, NY. After struggling to find reliable pediatric dental information during my own child’s dental emergency, I created this resource to help other Queens families navigate their children’s oral health needs.
I curate evidence-based information from leading pediatric dental organizations, peer-reviewed research, and trusted dental health experts. While I’m not a dentist, I’m committed to providing accurate, practical guidance that helps parents make informed decisions.
All content is thoroughly researched and includes proper medical disclaimers directing families to consult qualified pediatric dentists for their children’s specific needs.